
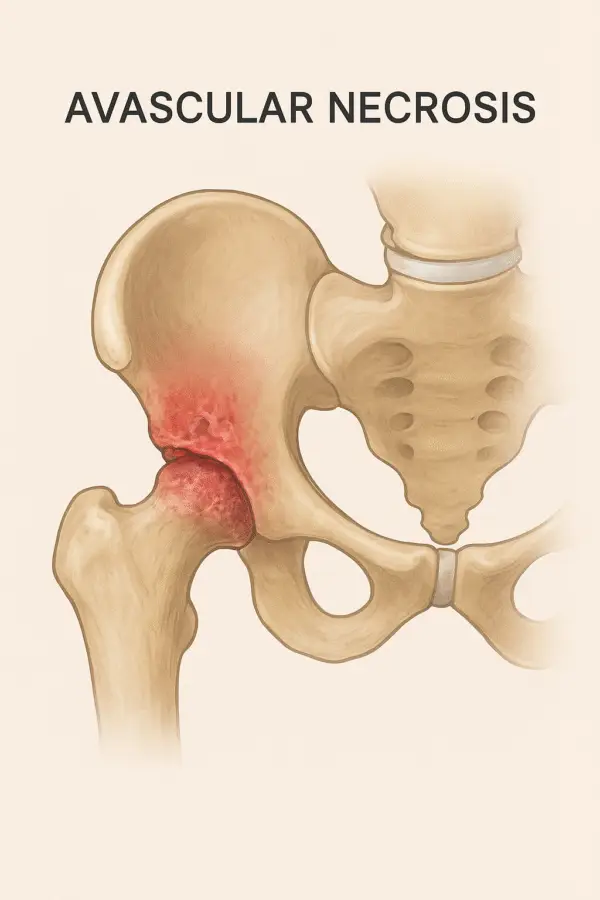
What is Avascular Necrosis?
Avascular necrosis (AVN), also known as osteonecrosis, is a medical condition in which bone tissue necroses due to a disruption in its blood supply. This lack of circulation leads to the gradual collapse of the bone structure, most commonly affecting the femoral head in the hip joint. If left untreated, AVN can lead to a significant joint impairment and the development of osteoarthritis..
Causes of Avascular Necrosis
The main cause of AVN is insufficient blood flow to the bone, which may occur due to multiple underlying factors:
- Trauma or Injury: Fractures or dislocations (especially in the hip) that damage surrounding blood vessels.
- Prolonged Corticosteroid Use: Long-term steroid medication can increase fat levels in the blood, leading to reduced blood supply.
- Excessive Alcohol Consumption: Alcohol interferes with the blood flow and increases fat deposits in the blood vessels.
- Medical Conditions:
- Sickle cell disease
- Autoimmune disorders
- Gaucher’s disease
- Radiation Therapy or Chemotherapy: Damage to blood vessels and bone tissue.
- Decompression Sickness: Rapid pressure changes in divers or pilots can cause gas bubbles to block blood vessels.
Signs and Symptoms of Avascular Necrosis
In its early stages, AVN typically progresses slowly and often presents without noticeable symptoms. As the disease progresses, common signs may include:
- Pain: Dull ache or throbbing pain in the affected joint (commonly hip, knee, or shoulder).
- Activity-Related Pain: Discomfort during weight-bearing activities such as walking or climbing stairs.
- Rest Pain: Pain at rest or even during nighttime in advanced stages.
- Limited Range of Motion: Difficulty moving the joint smoothly.
- Limping: Especially when the hip joint is affected.
Alleviating and Aggravating Factors
Aggravating Factors
- Prolonged standing or walking
- High-impact activities (running, jumping)
- Weight-bearing on the affected limb
Alleviating Factors
- Rest or non-weight-bearing positions
- Use of assistive devices (crutches or a cane)
- Application of heat therapy to relax the surrounding muscles
Objective Assessment in Avascular Necrosis
The goal of the Objective Assessment is to identify structural and functional impairments.
1. Observation
- Gait Pattern:
- Antalgic gait (due to pain)
- Limping if the hip is involved
- Posture:
- Decreased weight-bearing on the affected limb
- Compensatory trunk lean toward the affected side
- Muscle Atrophy:
- Thigh and gluteal muscles (due to disuse)
2. Palpation
Localized tenderness around the affected joint, particularly in the hip or groin area. Muscle tightness in the hip flexors or adductors.
3. Pain Assessment
- Location: Usually in the groin, thigh, or buttock (for hip AVN).
- Pain Characteristics:
- At Rest: Possible in later stages
- On Movement: Increases with weight-bearing or extremes of ROM
- Pain on Movement:
- Internal rotation and abduction are often painful
- Passive rotation can reproduce pain
4. Range of Motion (ROM)
- Active ROM:
- Limited due to pain, especially internal rotation and abduction.
- Passive ROM:
- Also restricted, but pain may appear earlier than the end range.
- Typical Findings:
- Internal rotation → Most restricted
- Abduction → Moderately restricted
- Flexion → Restricted in advanced stages
5. Muscle Strength Testing
- Weakness in hip abductors, extensors, and flexors due to pain and disuse.
- Manual Muscle Testing (MMT) is performed, but avoid excessive stress on the joint.
7. Functional Assessment
- Difficulty with:
- Walking
- Stair climbing
- Sitting-to-standing transitions
8. Gait Analysis
- Shortened stance phase on the affected limb.
- Trendelenburg sign may appear due to hip abductor weakness.
Rehabilitation Protocol for Avascular Necrosis
Rehabilitation strategies are determined by the severity and stage of AVN, as well as the extent of joint involvement. The primary goals are to reduce pain, maintain mobility, and delay joint replacement surgery.
1. Acute Stage (Early AVN)
- Rest & Offloading: Reduce weight-bearing using crutches or a walker.
- Pain Management:
- Heat therapy for muscle relaxation
- Cold therapy for acute pain
- Range of Motion Exercises: Gentle passive and active ROM to maintain joint flexibility.
2. Subacute Stage
- Strengthening Exercises:
- Isometric contractions of surrounding muscles (quadriceps, glutes)
- Core stabilization exercises
- Hydrotherapy: Reduces joint load while maintaining mobility.
- Low-Impact Aerobic Exercise: Swimming or cycling.
3. Advanced Stage
- Assistive Devices: Cane or walker for mobility.
- Activity Modification: Avoid high-impact activities.
- Joint Protection Techniques: Proper body mechanics during daily activities.
4. Post-Surgical Rehabilitation (Core Decompression or Joint Replacement)
- Early Phase: Gentle ROM exercises, pain control.
- Progressive Strengthening: Focus on hip abductors, extensors, and core muscles.
- Gait Training: To restore the normal walking pattern.
- Functional Training: Gradual return to daily and occupational activities.
Preventive Measures
- Limit alcohol consumption.
- Avoid long-term corticosteroid use unless medically necessary.
- Maintain a healthy weight to reduce joint stress.
- Manage chronic conditions such as diabetes and hyperlipidemia effectively.
Final Thoughts
Avascular necrosis is a progressive condition that can lead to severe disability if not diagnosed early. Timely medical intervention, lifestyle modification, and structured rehabilitation programs can significantly improve quality of life and delay the need for surgical interventions.


Sakıp Sabancı Museum tour Guides made the experience lively and enjoyable. https://concepcion.skincenter.cl/?p=6977
phqo1w