
Introduction
The shoulder is one of the most mobile joints in the human body, relying heavily on muscular stability. Among the four rotator cuff muscles, the subscapularis plays a crucial yet often overlooked role. It is the strongest and largest rotator cuff muscle, responsible primarily for internal rotation of the shoulder and anterior joint stability.
Injuries to the subscapularis tendon are increasingly recognized in clinical practice, especially among athletes, manual workers, and aging populations. However, due to subtle presentation, these injuries are frequently missed or misdiagnosed. This article explores subscapularis injury in detail, covering anatomy, causes, signs and symptoms, clinical presentation, diagnostic tests, and evidence-based rehabilitation protocols
Anatomy and Function of the Subscapularis
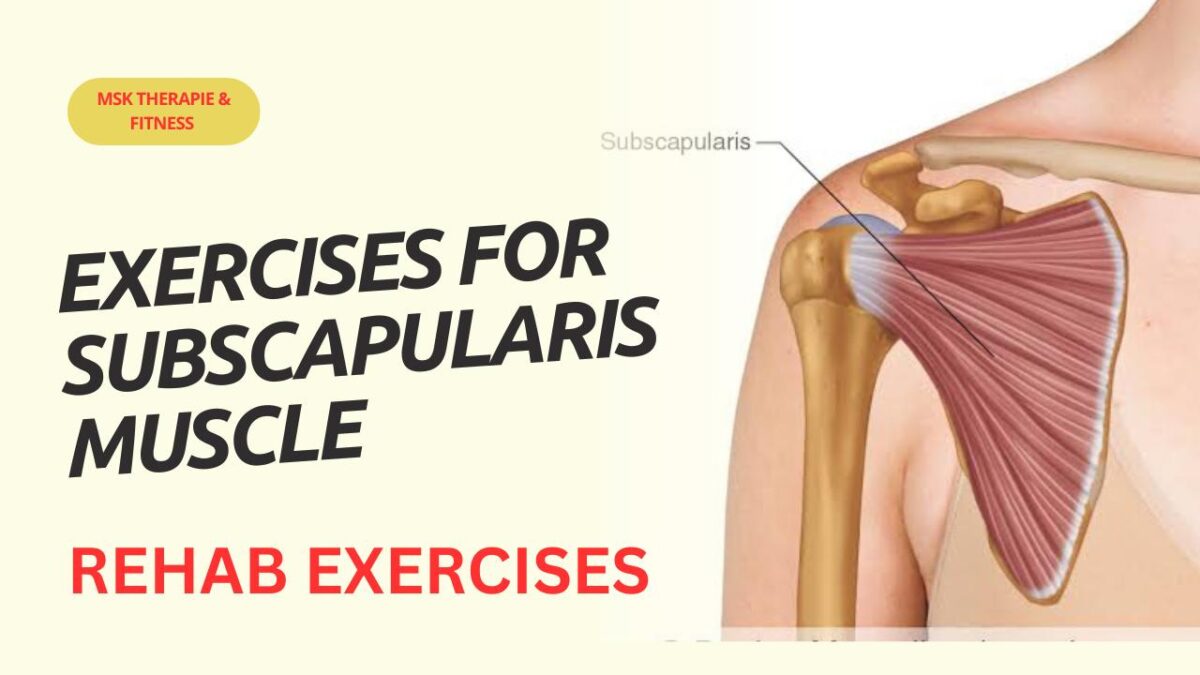
The subscapularis originates from the subscapular fossa of the scapula and inserts onto the lesser tuberosity of the humerus. It forms the anterior portion of the rotator cuff.
Primary Functions:
- Internal rotation of the shoulder
- Dynamic anterior stabilization of the glenohumeral joint
- Assists in adduction and depression of the humeral head
Because of its stabilizing role, injury can significantly compromise shoulder mechanics.
Causes of Subscapularis Injury
Subscapularis injuries may be traumatic or degenerative.
Common Causes:
- Acute trauma
- Fall on an outstretched arm
- Sudden external rotation force
- Shoulder dislocation
- Overuse
- Repetitive overhead activities (throwing, swimming, tennis)
- Occupational strain
- Degenerative changes
- Age-related tendon wear
- Poor vascularity
- Associated pathology
- Long head of biceps tendon instability
- Shoulder impingement
- Massive rotator cuff tears
Signs and Symptoms
Patients with subscapularis injury typically present with:
- Anterior shoulder pain
- Weakness during internal rotation
- Difficulty reaching behind the back
- Pain while pushing or lifting objects
- Clicking or catching sensation
- Night pain, especially when lying on the affected side
In complete tears, patients may report a sudden loss of strength following trauma.
Clinical Presentation
Observation
- Protective posture of the shoulder
- Muscle atrophy in chronic cases
- Altered scapular mechanics
Palpation
- Tenderness over anterior shoulder
- Pain near lesser tuberosity
Functional Limitations
- Reduced internal rotation range
Difficulty with daily activities (tucking shirt, fastening bra, reaching wallet)
Special Clinical Tests
1. Lift-Off Test
Patient places hand on lower back and attempts to lift it away.
Positive: Inability to lift hand = subscapularis tear.
2. Belly Press Test
Patient presses palm into abdomen while keeping elbow forward.
Positive: Elbow drifts backward = weakness.
3. Bear Hug Test
Patient places hand on opposite shoulder and resists examiner’s pull.
Positive: Inability to maintain position.
4. Internal Rotation Lag Sign
Examiner passively places shoulder in internal rotation.
Positive: Hand springs back = tendon insufficiency.
Rehabilitation Protocols for Subscapularis Injury
Rehabilitation depends on injury severity (conservative vs post-surgical). Below is a phased approach commonly used in physiotherapy practice.
Phase 1: Acute / Protection Phase (0–2 Weeks)
Goals:
- Reduce pain and inflammation
- Protect healing tissue
- Maintain mobility
Interventions:
- Activity modification
- Cryotherapy
- Pendulum exercises
- Passive ROM within pain-free limits
- Scapular setting
- Isometric internal rotation (sub-maximal)
Phase 2: Early Strengthening Phase (2–6 Weeks)
Goals:
- Restore ROM
- Begin muscle activation
- Improve scapular control
Exercises:
- Active-assisted ROM
- Theraband internal rotation
- Closed chain stabilization
- Serratus anterior activation
- Posterior capsule stretching
Phase 3: Progressive Strengthening Phase (6–12 Weeks)
Goals:
- Improve strength and endurance
- Enhance neuromuscular control
Exercises:
- Resistance band rotations
- Dumbbell internal rotation
- Prone rowing
- Scaption
- Proprioceptive drills
Phase 4: Functional / Return-to-Activity Phase (12+ Weeks)
Goals:
- Restore functional capacity
- Prevent recurrence
Training:
- Sport-specific drills
- Plyometric exercises
- Closed kinetic chain upper limb training
- Work conditioning
key exercises for subscapularis muscle
Internal rotation with resistance band
Exercise for subscapularis muscle
Exercise for subscapularis
Exercise for subscapularis
Prognosis
With early diagnosis and structured rehabilitation, outcomes are generally favorable. Delayed treatment may lead to chronic weakness, shoulder instability, and reduced function.
Prevention Strategies
- Proper warm-up before activity
- Balanced rotator cuff strengthening
- Scapular stabilization exercises
- Ergonomic workplace adjustments
- Avoiding repetitive overload
Conclusion
Subscapularis injuries are underdiagnosed yet clinically significant contributors to shoulder dysfunction. A thorough clinical examination combined with appropriate imaging ensures accurate diagnosis. Physiotherapy remains the cornerstone of management, whether conservative or post-surgical.
For clinicians, understanding specific test clusters and phased rehabilitation protocols is essential. For patients, early intervention dramatically improves recovery outcomes.


