
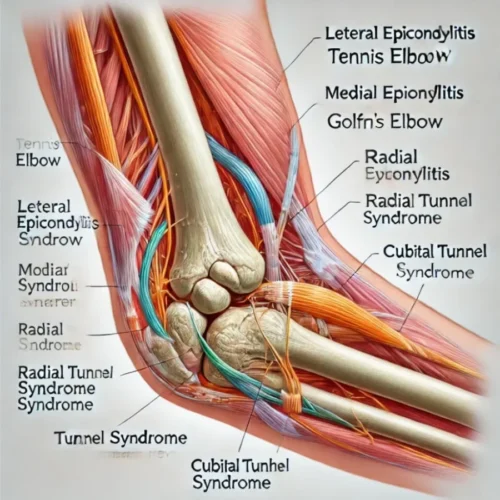
The elbow is a hinge joint comprising three bones the humerus, radius, and ulna. Elbow injuries are common and can result from trauma, overuse, or degenerative conditions. Elbow injuries often affect the muscles, tendons, ligaments, or joints, leading to pain, reduced range of motion, and functional limitations. Different types of elbow injuries such as lateral epicondylitis, medial epicondylitis, Cubital Tunnel Syndromes, and Radial Tunnel Syndrome are discussed in this blog.
Types of Elbow Injuries
Lateral Epicondylitis
Lateral Epicondylitis, commonly known as “Tennis Elbow,” is caused by overuse of the extensor muscles of the forearm, particularly the extensor carpi radialis brevis (ECRB). It causes pain on the outer side of the elbow.
Aggravating Factors of lateral epicondylitis:
- Repetitive wrist and forearm movements: Activities that involve excessive gripping, twisting, or lifting, such as tennis, typing, or manual labor.
- Resisted wrist extension or supination involves lifting with the palm facing down or gripping objects.
- Forceful gripping or pinching: Holding tools or objects tightly can aggravate the condition.
- Direct pressure on the lateral epicondyle: Pressure on the outer elbow region can increase pain.
- Repetitive elbow extension: Excessive elbow straightening movements.
Elevating (Relieving) Factor of lateral epicondylitis:
- Rest: Avoiding activities that provoke pain allows the tendon to heal.
- Ice therapy: Applying cold packs to the affected area can reduce inflammation and pain.
- Forearm bracing: Wearing an elbow brace or strap can offload stress from the affected tendon.
- Anti-inflammatory medication: NSAIDs like ibuprofen may temporarily relieve pain and inflammation.
- Stretching and strengthening exercises: Eccentric loading exercises for the wrist extensors can aid recovery when introduced progressively.
Diagnostic Tests for lateral epicondylitis:
Cozen’s Test (Resisted Wrist Extension Test):
- The patient’s elbow is flexed at 90 degrees, with the forearm pronated and the hand in a fist. The patient resists wrist extension. Pain over the lateral epicondyle suggests a positive result.
Mill’s Test:
- The examiner passively pronates the patient’s forearm, flexes the wrist, and extends the elbow. Pain at the lateral epicondyle during the movement indicates a positive test.
Maudsley’s Test (Resisted Middle Finger Test):
- The patient resists extension of the middle finger while the elbow is extended. Pain over the lateral epicondyle is a positive result, indicating stress on the extensor muscles.
Chair Test:
- The patient tries to lift a chair with their forearm in pronation and elbow extended. If this action reproduces pain, the test is positive.
Physiotherapy Treatment for lateral epicondylitis:
- Rest and Activity Modification: Initially, avoiding aggravating activities (gripping, lifting) is recommended.
- Manual Therapy: Soft tissue massage, mobilizations, and myofascial release to reduce tension in the extensor or flexor muscles.
- Stretching Exercise: For lateral epicondylitis, wrist flexor stretches are while for radial epicondylitis extensor stretches are effective.
- Strengthening Exercises:
- Eccentric exercises: Particularly effective for tendinopathies, focusing on slow and controlled lowering movements.
- Grip Strengthening: using hand grippers or squeezing putty.
- Electrotherapy: Use of ultrasound therapy or TENS (Transcutaneous Electrical Nerve Stimulation) to relieve pain and promote healing.
- Icing and Heat Therapy: Ice for inflammation, heat for muscle relaxation.
Medial Epicondylitis
Medial Epicondylitis, commonly known as Golfer’s Elbow, is a condition characterized by pain and inflammation of the tendons that attach to the medial epicondyle of the elbow. It primarily affects the forearm flexors and pronator muscles, such as the flexor carpi radialis and pronator teres.

Aggravating Factors:
- Repetitive wrist flexion or forearm pronation: Activities involving frequent bending of the wrist or rotating the forearm inward, like golfing, throwing, or lifting objects with the palm facing upward.
- Forceful gripping or squeezing: Tasks that involve a strong grip, such as shaking hands, lifting heavy objects, or using tools.
- Resisted wrist flexion or pronation: Engaging in resisted exercises where the wrist or forearm flexes can provoke pain.
- Activities that involve elbow flexion and wrist flexion simultaneously: Movements like picking up heavy objects, driving screws, or using hand tools.
- Direct pressure on the medial epicondyle: Pressing on the inner side of the elbow or resting the arm on hard surfaces.
Elevating (Relieving) Factors:
- Rest: Avoiding repetitive wrist or elbow movements allows the irritated tendons to recover.
- Ice therapy: Applying ice to the affected area can help reduce pain and inflammation.
- Stretching and gentle strengthening exercises: Stretching the forearm flexor muscles and gradually strengthening them can alleviate pain over time.
- Forearm bracing: Wearing a counterforce brace or strap may relieve stress on the tendons, providing support.
Diagnostic Tests:
Golfer’s Elbow Test (Resisted Wrist Flexion):
- The patient’s elbow is flexed at 90 degrees with the forearm supinated. The examiner applies resistance and the patient resists wrist flexion. Pain at the medial epicondyle is a positive sign.
Passive Forearm Supination and Wrist Extension Test (Stretch Test):
- The examiner passively supinates the patient’s forearm and extends the wrist and elbow. Pain at the medial epicondyle during this stretch indicates a positive result.
Palpation of the Medial Epicondyle:
- Direct palpation of the medial epicondyle area elicits tenderness in cases of Golfer’s Elbow.
Resisted Pronation Test:
- The patient resists pronation (turning the palm downward) while the examiner applies resistance. Pain over the medial epicondyle suggests a positive test.
Physiotherapy Treatment:
- Rest and Activity Modification: Initially, avoiding aggravating activities (gripping, lifting) is recommended.
- Manual Therapy: Soft tissue massage, mobilizations, and myofascial release to reduce tension in the extensor or flexor muscles.
- Stretching Exercise: For medial epicondylitis wrist extensor stretches are effective while for lateral epicondylitis flexor stretches are effective.
- Strengthening Exercises:
- Eccentric exercises: Particularly effective for tendinopathies, focusing on slow and controlled lowering movements.
- Grip Strengthening: using hand grippers or squeezing putty.
- Electrotherapy: Use of ultrasound therapy or TENS (Transcutaneous Electrical Nerve Stimulation) to relieve pain and promote healing.
- Icing and Heat Therapy: Ice for inflammation, heat for muscle relaxation.
Cubital Tunnel Syndromes
It is a condition caused by compression or irritation of the ulnar nerve as it passes through the cubital tunnel, a narrow space on the inside of the elbow. This nerve compression can result in a variety of symptoms, including numbness, tingling, and weakness in the hand and arm. The ulnar nerve controls sensation in the ring and little fingers and helps with the fine motor function of the hand.
Signs and Symptoms:
- Numbness and tingling: Numbness and a “pins and needles” sensation often occur in the ring finger and little finger, especially after the elbow is bent for long periods.
- Pain in the elbow: Pain or aching may occur on the inside of the elbow, especially after prolonged use or resting on the elbow.
- Wartenberg sign: presence of wartneberg sign. Wartenberg sign is the abduction of the fifth digit due to weakness of the third palmar interosseous muscle.
- Weakness in the hand: Weakness in the grip or difficulty with fine motor skills (e.g., typing, writing, or playing instruments) due to impaired control of the hand muscles, particularly the intrinsic hand muscles.
- Clawing of the ring and little fingers: In more severe cases, the muscles controlling the ring and little fingers may weaken, causing these fingers to curl into a claw-like position (ulnar claw hand).
- Loss of coordination: Difficulty coordinating hand movements, such as buttoning a shirt or handling small objects.
- Pain or discomfort when bending the elbow: Symptoms are often worse when the elbow is bent, such as during activities like talking on the phone or sleeping with the arm curled up.
Aggravating Factors:
- Prolonged elbow flexion: Keeping the elbow bent for long periods (e.g., while talking on the phone, driving, or sleeping) puts pressure on the ulnar nerve and increases symptoms.
- Repetitive elbow movements: Activities involving frequent bending and straightening of the elbow (e.g., lifting, throwing, or typing) can irritate the ulnar nerve.
- Direct pressure on the inner elbow: Leaning on the elbow, resting it on hard surfaces, or placing pressure on the cubital tunnel area can aggravate symptoms.
- Trauma or elbow injury: Previous elbow injuries, such as fractures or dislocations, can worsen or trigger symptoms.
Elevating (Relieving) Factors:
- Avoiding prolonged elbow flexion: Keeping the elbow straight, especially while sleeping, can reduce pressure on the ulnar nerve. Wearing an elbow splint to prevent bending at night is often helpful.
- Using padding or cushioning: Wearing an elbow pad or cushioning when leaning on hard surfaces can help reduce pressure on the ulnar nerve.
- Rest and activity modification: Reducing repetitive elbow movements or resting the arm can help alleviate symptoms.
- Stretching and nerve gliding exercises: Specific exercises designed to mobilize the ulnar nerve and stretch the surrounding muscles can help reduce compression.
Diagnostic Tests:
Tinel’s Sign (at the elbow):
- The examiner taps gently over the ulnar nerve at the elbow (just behind the medial epicondyle). If tapping produces tingling or a “pins and needles” sensation in the ring and little fingers, this is considered a positive Tinel’s sign for Cubital Tunnel Syndrome.
Elbow Flexion Test:
- The patient bends the elbow fully and holds it in this position for 1-3 minutes. If numbness or tingling develops in the ring and little fingers during this time, the test is positive for ulnar nerve compression.
Froment’s Sign:
- The patient attempts to hold a piece of paper between the thumb and index finger while the examiner pulls it away. In cases of ulnar nerve dysfunction, the patient may compensate by flexing the thumb’s interphalangeal joint, indicating weakness in the adductor pollicis muscle.
Scratch collapse test:
- Slightly scratch the patient skin over the area of nerve compression and resist bilateral shoulder external rotation. A positive test is indicated by a brief collapse or loss of resistance, which suggests ulnar nerve irritation.
Nerve Conduction Study (NCS):
- A nerve conduction test measures the speed at which electrical signals pass through the ulnar nerve. A slowed signal across the elbow indicates nerve compression.
Physical therapy treatment:
- Nerve Gliding Exercises: To reduce nerve compression and promote mobility.
- Splinting or Bracing: Especially during the night, to prevent excessive flexion of the elbow in cubital tunnel syndrome.
- Activity Modification: Avoid prolonged elbow flexion, direct pressure on the elbow, or repetitive activities that exacerbate symptoms.
- Strengthening Exercises: Once pain decreases, focus on strengthening the muscles around the elbow and forearm.
- Electrotherapy: To manage nerve pain and promote healing.
Olecranon Bursitis
It is also known as “student’s elbow“. Olecranon Bursitis is the inflammation of the bursa located over the olecranon (the bony prominence at the back of the elbow). The bursa is a small fluid-filled sac cushioning the bones, tendons, and muscles near the joint, and inflammation causes swelling and discomfort. Here’s a detailed overview of the signs, symptoms, aggravating factors, elevating factors, and diagnostic tests:
Signs and Symptoms:
- Swelling: One of the most noticeable signs is swelling at the back of the elbow, which can be soft or firm. The swelling may grow gradually or appear suddenly.
- Pain: The elbow may be painful to the touch, particularly with pressure on the swollen area. Pain can be mild or severe, depending on the degree of inflammation or infection (if present).
- Redness and warmth: The skin over the bursa may appear red, warm, or hot, indicating possible infection (septic bursitis).
- Restricted range of motion: Swelling can limit movement at the elbow, making it difficult to fully bend or straighten the arm.
- Pus drainage (if infected): In cases of septic bursitis, the bursa may become infected, leading to the accumulation of pus. This may cause the skin to break, and pus could drain out.
- Tenderness: The area over the olecranon may be tender to the touch, especially during movement or direct pressure.
Physical therapy treatment:
- Rest and Ice: To reduce swelling.
- Compression: Apply a compression bandage to limit further swelling.
- Range of Motion Exercises: To maintain elbow flexibility, particularly once the inflammation subsides.
- Education: Advising patients to avoid leaning on their elbows or repetitive pressure on the joint.
Radial Tunnel Syndrome
Radial Tunnel Syndrome, is a condition caused by compression or irritation of the radial nerve as it passes through the radial tunnel, located near the elbow and forearm. This syndrome often mimics tennis elbow (lateral epicondylitis) but involves a different structure — the radial nerve — which supplies motor and sensory functions to parts of the arm and hand.
Signs and Symptoms:
- Deep, aching pain in the forearm: Pain is often located about 2 to 4 centimeters below the lateral epicondyle (outer part of the elbow) and can extend down the forearm. It is usually described as a deep, aching pain, rather than sharp.
- Pain with forearm and wrist movements: Symptoms are aggravated by activities involving repetitive forearm rotation (supination and pronation) or wrist extension, such as turning a doorknob, using a screwdriver, or lifting objects.
- Pain that worsens with elbow extension and forearm rotation: Actions like extending the elbow while rotating the forearm can increase discomfort.
- Weakness in the forearm: Although muscle weakness is less common than in other nerve compression syndromes, patients may report a feeling of weakness in the hand or forearm.
- Tenderness on palpation: Tenderness is typically felt in the area about 3-5 cm distal to the lateral epicondyle, over the radial nerve pathway. Unlike lateral epicondylitis, pain is more diffuse and deeper.
- Lack of sensory loss: Sensory deficits like numbness or tingling in the fingers are uncommon in radial tunnel syndrome, as the radial nerve primarily supplies motor function to the extensor muscles of the forearm.
Diagnostic Tests:
Middle Finger Test (Resisted Third Finger Extension Test):
- The patient extends the middle finger against resistance while keeping the elbow extended. A positive test reproduces pain in the area of the radial tunnel, near the lateral epicondyle.
Radial Tunnel Compression Test:
- The examiner applies pressure over the radial tunnel (just below the lateral epicondyle) while the patient’s arm is in extension. If this reproduces pain, it suggests radial nerve compression.
Forearm Supination Test:
- The patient resists forearm supination (turning the palm upwards) with the elbow extended. If this movement causes pain near the radial tunnel, it indicates radial nerve involvement.
Palpation of the Radial Tunnel:
- Tenderness or pain on pressing over the radial nerve in the radial tunnel (about 3-5 cm distal to the lateral epicondyle) is a common finding.
key differences between radial tunnel syndrome, lateral epicondylitis, and cubital tunnel syndrome.
- Unlike lateral epicondylitis, where the pain is directly over the lateral epicondyle, the pain in radial tunnel syndrome is located just below it, deeper in the forearm.
- Unlike cubital tunnel syndrome or other nerve entrapments, there is typically “no sensory loss” or numbness associated with radial tunnel syndrome because the radial nerve compression here does not affect the cutaneous sensory branches.
Physical therapy treatment:
- Nerve Gliding Exercises: To reduce nerve compression and promote mobility.
- Splinting or Bracing: Especially during the night, to prevent excessive flexion of the elbow in cubital tunnel syndrome.
- Activity Modification: Avoid prolonged elbow flexion, direct pressure on the elbow, or repetitive activities that exacerbate symptoms.
- Strengthening Exercises: Once pain decreases, focus on strengthening the muscles around the elbow and forearm.
- Electrotherapy: To manage nerve pain and promote healing.
General Physiotherapy Modalities
- Manual Therapy: Techniques such as joint mobilizations, soft tissue release, and manipulations can help reduce stiffness and improve mobility.
- Electrotherapy: Ultrasound, TENS, or interferential current therapy can help in reducing pain and inflammation.
- Therapeutic Exercises: Stretching, strengthening, and proprioception exercises tailored to the specific injury help restore function.
- Kinesio Taping: Supports the muscles, tendons, and ligaments while allowing movement.
- Hydrotherapy: Using water-based exercises to gently restore motion and strength.
Prevention Strategies
- Ergonomics: Proper techniques in sports, work, or daily activities to avoid repetitive stress or strain on the elbow.
- Strengthening: Maintaining strength in the shoulder, forearm, and hand muscles can offload stress from the elbow.
- Stretching: Regular stretching of the forearm muscles can prevent tendinopathies like tennis or golfer’s elbow.
- Warm-up and Cool-down


It’s going tto bbe nding off mine day, except befokre
eding I amm readingg this fantasstic piecfe of
writing too improve myy knowledge.
0tksaz
I am regular visitor, how are you everybody? This article posted at this web site is truly fastidious.